


Oral Cancer
Course Number: 348
Treatment
If the pathologist reports the lesion as cancer, then the patient should be referred promptly to a cancer treatment center for assessment and treatment. An important component of the assessment is to establish the stage of the disease. Similar to cancers at other sites in the body, cancer of the mouth is staged using the TMN system where T stands for tumor size, N for the presence or absence of tumor involvement in regional lymph nodes and M for the presence or absence of distant metastases. Generally, the prognosis is better when the tumor is smaller and has not metastasized to either lymph nodes or other organs. Staging also plays an important role in determining the most appropriate therapy for cancer of the oral cavity. An important exception is that tumors associated with HPV infection have a markedly better survival rate.
Cancer of the oral cavity is treated by:
Surgery
Radiation therapy
Chemotherapy is often added to either treatment. Adjuvant therapies such the use of antibodies directed against certain cancer associated antigen (e.g. anti-EGFR therapies) and immunotherapies that activate the patient’s immune system lymphocytes to target and kill the tumor (so-called check point inhibitors) are increasingly used in many human cancers including those arising in the oral cavity.
For cancers that are restricted to the oral cavity, surgery is generally the preferred treatment modality. Depending on the site, small lesions can be excised and closed primarily. Larger lesions may require more complicated surgical reconstruction using grafting material taken from the arm or the leg. For patients with bulky tumors or for those with tumor in regional lymph nodes, the preferred treatment is radiotherapy. In these instances, radiation is administered in small daily doses (fractions) of about 2 Grays until a total dose of about 70 Gray has been administered. Radiation therapy has the effect of destroying the salivary glands and reducing the vascularity to the mandible and maxilla. Hence, patients who have had radiation therapy to the head and neck have a life-time risk of developing a form of osteomyelitis, termed osteoradionecrosis of the jaws (Figures 6, 7).

Figure 6. Osteoradionecrosis of the mandible. This patient had received radiation therapy for a tongue SCC in the past.
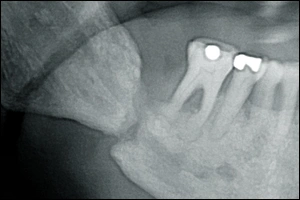
Figure 7. This radiograph shows a pathologic fracture of the mandible secondary to osteoradionecrosis. The patient had received radiation therapy to the oral cavity in the past.
Frequently, osteoradionecrosis is precipitated by dental extractions to an irradiated jaws, therefore, special methods are employed in these individuals when dental extractions are planned.7 Usually, any tooth which might be anticipated to need extraction in the future is extracted prior to radiation therapy. Cancer of the lip is usually by surgery alone. Carcinoma of the oropharynx that is associated with HPV responds well to radiation and chemotherapy.