


Management of Pediatric Medical Emergencies in the Dental Office
Course Number: 391
Course Contents
Cardiac Arrest
Every year, around 350,000 people in the United States suffer from cardiac arrest and receive attempted resuscitation. Cardiac arrest, although common in adults, is a rare occurrence in the pediatric population. When it does occur, the outcome can be devastating. Death may result or if the patient is not resuscitated on time, permanent brain damage may occur. The etiology of cardiac arrest in a child differs from an adult. Cardiac arrest in the pediatric patient is the result of prolonged respiratory depression and apnea. These situations are often associated with local anesthesia toxicity because of overdose or intravascular injection and with the administration of CNS depressant drugs for behavior management.
Comprehensive BLS training is not within the scope of the course, and it is recommended the reader seek out formal BLS instruction. The etiologies for cardiac arrest differ for adults (cardiac disease) and children (depleted oxygen in the myocardium). For unwitnessed and witnessed cardiac arrests with two or more rescuers present, assess the patient, initiate CPR, activate the emergency response system and obtain an automated external defibrillator (AED) simultaneously.
For unwitnessed and witnessed cardiac arrests with two or more rescuers present, assess the patient, initiate CPR, activate the emergency response system and obtain an automated external defibrillator (AED) simultaneously.
For the lone rescuer, the sequence varies:
If the cardiac arrest is witnessed, the lone rescuer first activates the emergency response system, obtains an AED, and starts CPR. This approach is the same as for adult with cardiac arrest.
If the cardiac arrest is unwitnessed, the lone rescuer should first perform two minutes of CPR, activate the emergency response system, and obtain an AED.
This approach differs from that recommended for adult cardiac arrest, which is call for help, activate the emergency response system and initiate CPR and obtain an AED.
For the summary of high-quality CPR for infants, children, and adolescents, kindly refer to American Heart Association guideline (Figure 19).
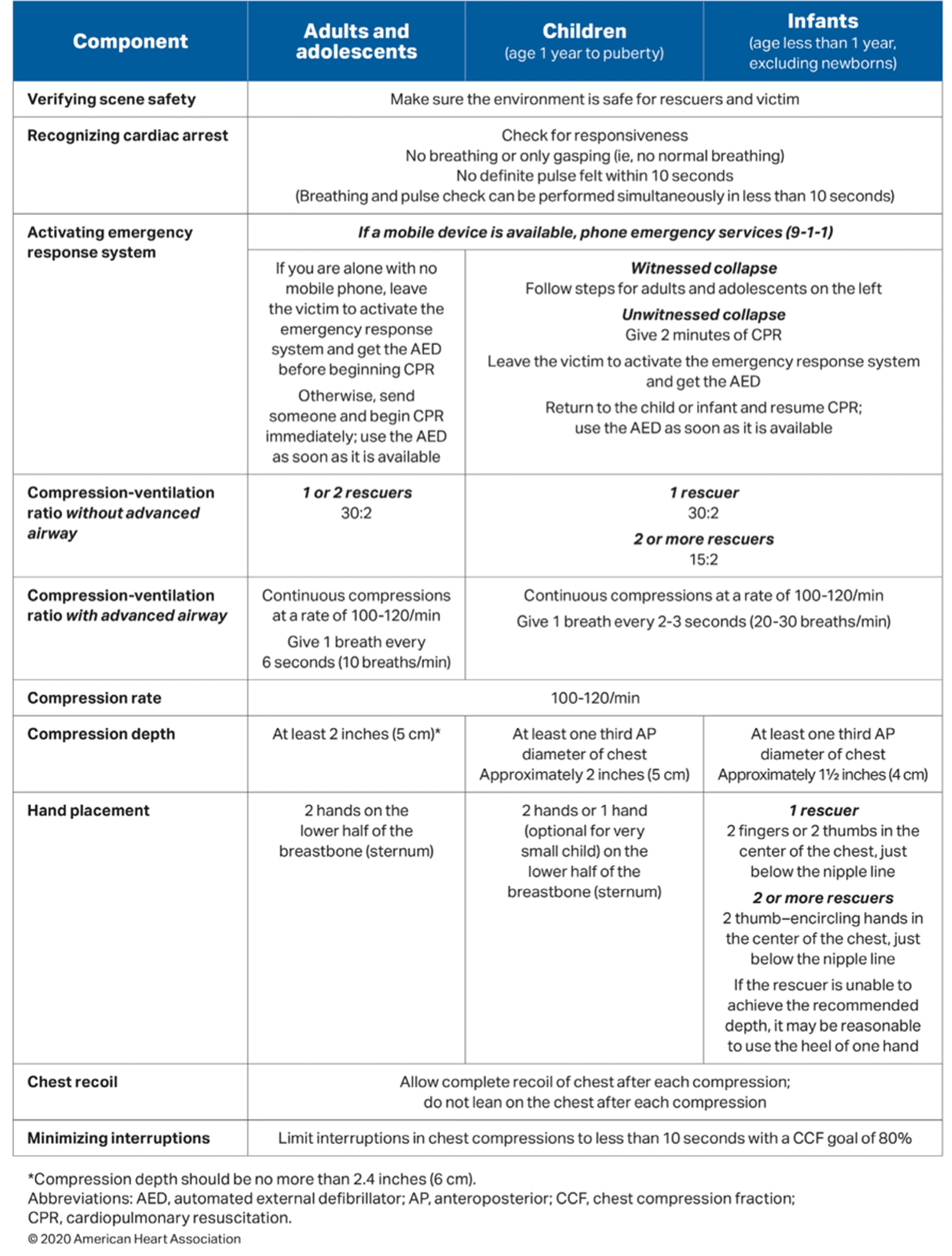
Figure 19. Summary of high-quality CPR components for BLS providers.21
Comprehensive CPR training is not within the scope of this course, and it is recommended the reader seek out formal BLS instruction. It is important for BLS providers to realize because of different etiologies for cardiac arrest in adults (cardiac disease) and children (depleted oxygen in the myocardium) there is a significant difference in BLS protocols for adults and children. In adults, after initial assessment of the unresponsive patient, EMS is activated immediately (before starting BLS) so access to trained personnel and defibrillation equipment is available as soon as possible. In children, since the likely cause of cardiac arrest is lack of oxygen in cardiac muscle, BLS is started immediately, and EMS is contacted after delivery of BLS for 2 minutes.